Sign up for our monthly Leap Update newsletter and announcements from the Leap Ambassadors Community:
By clicking "Stay Connected" you agree to the Privacy Policy
By clicking "Stay Connected" you agree to the Privacy Policy

Our Common Definition of High Performance
Without a thoughtfully developed, thoroughly vetted definition of “high performance,” any call for raising performance in our sector rings hollow.
Definition
Courageous, Adaptive Executive and Board Leadership
Leadership, the preeminent pillar of high performance, helps your organization embark on a journey to make it even stronger.
Practice Imperative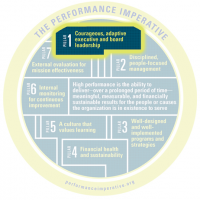
Disciplined, People-Focused Management
Join forces to make your disciplined and people-focused management even stronger.
Practice Imperative
Well-Designed And Well-Implemented Programs And Strategies
Well-designed and well-implemented programs help the people and causes you serve.
Practice Imperative
Financial Health And Sustainability
Get on the path to long-term financial sustainability.
Practice Imperative
A Culture That Values Learning
Double down on developing a culture that values learning.
Practice Imperative
Internal Monitoring For Continuous Improvement
Internal data help you make decisions that leads to continuous improvement.
Practice Imperative
External Evaluation For Mission Effectiveness
External evaluation can help you ensure mission effectiveness.
Practice Imperative
Samantha Sherrod • January 2023
 For nearly 40 years, Leap Ambassador A. Toni Young has been on the frontlines of efforts to end the HIV/AIDS epidemic. Toni is the founder and executive director of the Community Education Group (CEG), which provides access to healthcare, public education, job training, and economic opportunity for underserved rural communities and community-based organizations in broader Appalachia.
For nearly 40 years, Leap Ambassador A. Toni Young has been on the frontlines of efforts to end the HIV/AIDS epidemic. Toni is the founder and executive director of the Community Education Group (CEG), which provides access to healthcare, public education, job training, and economic opportunity for underserved rural communities and community-based organizations in broader Appalachia.
As an African American, bisexual woman, she’s constantly exploring what equity looks like through many lenses. Leap support team member and ambassador Samantha Sherrod spoke with Toni about why she moved from Washington, DC to Charleston, WV, how her professional passion evolved to focus on equipping rural, white communities with the resources needed to help people achieve optimal health and well-being, and what she thinks others should know about the people of Appalachia.
Toni: In 1991, when my best friend, Steven, was dying from HIV/AIDS, he said, “One day, this disease is going to look more like you. You need to figure out what you’re going to do on behalf of people who look like you.” At that point, I had worked on one of the first AIDS vigils at the White House and on the National Mall. I had fundraised for HIV/AIDS awareness and prevention groups and volunteered with the Whitman Walker Hotline, now Whitman-Walker Health, when it went from the “LGBT suicide line” to the “drip hotline” to the “AIDS hotline.” Then, I worked for the National Women’s Health Network as an HIV and internship coordinator. While there, I kept pushing the agenda around women and HIV, because it was impacting women of color. Although I insisted that HIV is related to women’s health, the women they perceived to be impacted by HIV were not a part of their membership, which were middle-aged, wealthier white women who didn’t see themselves at risk or in this fight.
I decided to put my energy into women, people of color, and HIV work. In 1994, I quit my job, and with my unemployment check founded the National Women’s HIV/AIDS Project, which was the original name of what we now know as the Community Education Group (CEG). We primarily served Southeast DC, and, with a friend’s help, I wrote my first proposal to Design Industry Funders in the Fight Against AIDS, who gave us $10,000, our first grant.
Toni: While living and working in my hometown of Southeast DC, I bought a house in West Virginia. It was supposed to be my weekend retreat, where I would de-stress and write books, including one about the AIDS movement. One day in 2015, while I was sitting on my porch minding my business, Corinna Dan, who worked at the United States Department of Health and Human Services, sent me the Centers for Disease Control (CDC) Morbidity and Mortality Weekly Report on the 220 most vulnerable counties in the United States and a Wall Street Journal article about the direct correlation of the opioid epidemic in West Virginia and the increase in Hepatitis C. I learned that 28 of West Virginia’s 55 counties were among the most vulnerable. Also, I was reminded that West Virginia and Kentucky were ranked number one and two, respectively, for over a decade in Hep C rates. I thought: HIV is next. But because we are 30 years into an epidemic, no one else is seeing this population in that way.
When I say, “Parts of West Virginia have a higher rate of HIV due to intravenous drug use than New York City,” people are befuddled. I use this analogy: There’s a train running not just through West Virginia but through all of Appalachia, and the engine of that train was injection drug use. Then, it became polydrug use. The next train cars are Hep C, Hep A, economic development, workforce development, and educational-attainment challenges, with the caboose being HIV. Also, in each of those cars is the impact of coal, strip mining, and other environmental issues. So we have to do a lot of work really fast in this part of the country.
Toni: The Appalachian region spans 423 counties across 13 states [including parts of Alabama, Georgia, Kentucky, Maryland, Mississippi, New York, North Carolina, Ohio, Pennsylvania, South Carolina, Tennessee, and Virginia, and all of West Virginia]. The Appalachian Mountains also extend into Maine, Massachusetts, New Hampshire, and Vermont. But those states are not framed in the “423 counties of the Appalachia region” as defined by the Appalachian Regional Commission, because they are wealthier areas.
Within those 423 counties, there’s a culture. People don’t want anyone from the outside telling them what to do. Most people in this part of the country have been here for seven to 10 generations. The young people leave, but the older people stay. So we’ve got to figure out how to strategically get information into the region in a way that is culturally responsive. We cannot say, “We’ll give you information this way; it’s from X place, and you have to take it.” We’re approaching the work differently and determining how to train people in this region so they can give others information.
Toni: People are always shocked that I talk about people in Appalachia. I think people see what they want to see. They might see me as queer, lesbian, butch, or a left-of-center person doing this work. I don’t think of myself like that. I think of myself as a public health professional living and working in a rural community. My project “We Are Appalachia” involves looking at the academic study of Appalachia over the last 30 years and figuring out the region’s challenges based on poverty and culture. This is not an issue of color. This is an issue of getting the people of Appalachia healthy, happy, and whole. We can do that by deconstructing the silos of public health, economic development, and workforce development.
Many people spend their entire lives asking why God put them on the planet. I know why God put me here: to help other people, whether doing HIV/AIDS work with returning citizens in Southeast DC or working in Appalachia on the dual syndemics of HIV, HCV (Hepatitis C virus), and substance use disorders on one end and poverty, environmental challenges, and economic barriers on the other. These dual syndemics often collide and lead to poor health, environmental and economic outcomes.
At moments in my life, I have felt the presence of Steven and others I met along the way. They tell me: “Go! Don’t do it that way. Look over there and do it that way.” Sometimes it can look like I’m walking through the world like I know what I’m doing. That’s not the case. My friends just told me what to do. And so that’s what I do.
Toni: CHAMPS is a hybrid of a community health worker model and peer education model. The key to CHAMPS in DC was to have folks from the community do HIV and Hep C testing and link people to care. We wanted to disprove the notion that people wouldn’t test or share personal health information with people they know. We thought that if you see a person who’s had the same lived experiences as you doing this work, it’s a more trusting environment. This person gets you.
The beauty of the CHAMPS program in DC was that we set up “red carpet care” with other providers in the region, so that when people tested positive for HIV or Hep C, they could immediately connect with the care they needed. That’s what got our testing numbers up and helped us achieve a care rate of 96 percent.
With the CHAMPS program in DC, we relied heavily on individuals with histories of incarceration, because they needed jobs and were almost guaranteed to show up and do the work. When applying to the CHAMPS program, some people had resumes. For those who didn’t, we had staff to help them. We wanted them to treat this as their first opportunity back into the workforce. Over a 90-day period, we trained and paid the workers. For those who weren’t accepted into CHAMPS, we helped them find employment. We always had more applicants than slots for each round.
Last year, we got the chance to hear about the program’s impact from nine previous CHAMPS participants. Each has found gainful employment. All of them said that they felt like the program gave them a shot. A CHAMPS alum who now works at the Library of Congress said, “I was 30-something-years-old coming into CHAMPS, and I had never had a job in my life. If I didn’t work at CHAMPS, I wouldn’t have the job I have now.” That focus group was the moment I saw our impact.
Toni: In West Virginia, we have two challenges with the CHAMPS model. One, we’re still coming out of COVID, so we’re thinking about our approach to the training. Do we do in-person, hybrid, or electronic? If we do electronic and hybrid, we have to worry about who does and doesn’t have access to broadband. If we do brick and mortar, we must have at least seven locations to create a hub for all 55 counties across the state. We’ve landed on an LMS [Learning Management System] for training. People will have the option to go to the library, do all work on their phone, or attend live classes.
Two, unlike CHAMPS in DC, we have a limited number of healthcare providers. We are educating Congress, public health officials, and the federal government about the needs of the people of Appalachia. Because they are forgotten people. If you can forget poor white people, the jig is up. So, we’re developing new partnerships. We are working with Members of Congress, including United States Senators Shelley Moore Capito (R-WV) and Joe Manchin (D-WV), who asked Dr. Rochelle Walensky, director of the CDC, “Where is West Virginia’s money for ending the HIV epidemic?”
We’re also working with the National Rural Health Association and others to create an Office on Rural Health at the CDC. We want to make this office happen for the entire Appalachian region, as it’s critically important to the health and the outcomes of the region. We’re also collaborating with YAP [Youth Advocate Programs], where Leap Ambassador Gary Ivory is the president, to create an exchange program between organizations in Appalachia and YAP’s international partners in Sierra Leone, Guatemala, Mexico, and Ireland. The program will allow the organizations’ executive directors, program staff, and program participants to learn from each other about how to improve the health of their local communities.
Toni: People look at me and think that it’s about racial equity. But that’s not our fight right now. The work we’re doing in the Appalachian region is about equitable health access, health outcomes, and participation in a healthcare system. In the Appalachian region, we’re dealing with an issue of cultural equity which means that the culture of the Appalachian region will be valued and, as a result, the people will receive their fair share of health education and economic development inputs. We are trying our hardest to get programs and services into the “hollers” [a sheltered valley between mountains] where people live. We are also working on getting resources to provide people with the health education and training they need to succeed.
It’s great that West Virginia expanded Medicaid so more people have insurance coverage for healthcare. But where are the providers? Also, the infrastructure they need is missing. I could build a rural hospital here, but I would have to construct a road to get to the hospital. The hospital has to get broadband to access electronic health records, and so do people’s homes, so those who don’t have a car can access telehealth. Then I have to figure out how to attract the professionals to work in the hospital, because they can make two-thirds more across the border in DC, Virginia, and Maryland. So we have to figure out so much more to address healthcare. And that costs.
Advancing equity for the people of Appalachia means every Notice of Funding Opportunity (NOFO), [which is the way the federal government solicits applications for grant funds for a specific project according to eligibility criteria] should include the 423 counties of the Appalachian region. Because the people of Appalachia have not been able to get their just due. Also, nearly half of the 423 counties (44 percent or 187 counties) touch more than one state. We need to figure out a way to give the people of Appalachia access to federal monies that they can move across state lines. Most federal grants require projects to declare a state or county boundary. If this stipulation were allowed in a NOFO, more than one area could benefit from a federally funded project.
Toni: More than anything, I want people to know that life in Appalachia is not what you see on TV. It’s not that folks are race-hating, race-baiting individuals. We must understand that there are people in Appalachia who are poor, the majority of them are white, and living in trailers and “hollers”. We’ve got to figure out how we’re going to get information into these hollers and put energy into discovering where there are broadband outages.
There is a great need in the Appalachian region. We need resources for organizational development, capacity building, and “old school” mobilization efforts. We need to figure out how to get medication-assisted treatment providers trained so that they understand that they sit at the nexus of so much. For example, when providers respond to a substance-use disorder, they also have an opportunity to do HIV and Hep C testing, workforce development, economic development, and anything you can think of to help families. So we’ve got to get them the capacity-building services that they need and the skills that they need in order to better serve this population. But because they haven’t historically been seen as a critical partner in our response to public health and economic development, it’s been a challenge.
We need a major investment in this region of the country—in health, education, economic development, and workforce development—to ensure that the people and communities of Appalachia survive and ultimately thrive.
Friends and colleagues inspired Toni to find ways to fight the HIV/AIDS epidemic in Southeast DC and, more recently, in West Virginia. With a firm belief in who she is and a commitment to the public health profession, Toni has discerned that cultural inequity has negatively impacted the health outcomes of Appalachian residents. She is as an ally to the people of Appalachia as she fights to dismantle cultural injustice to improve the quality of life for all in the region.
The Leap of Reason Ambassadors Community is a private community of experts and leaders who believe that mission and performance are inextricably linked. Our resources are collaboratively developed and offered to the field to support organizations on their journeys to high performance.
We use cookies for a number of reasons, such as keeping our site reliable and secure, personalising content and providing social media features and to analyse how our site is used.
Accept & Continue